Osteoporosis
Osteoporosis is a chronic disease of bone metabolism, in which there is a gradual decrease in their density and quality, resulting in them becoming more fragile over time and consequently an increased risk of fractures, especially in the spine, hip area and other bones.
Osteoporosis usually occurs after the age of 50 and is much more common in women than in men, with its frequency increasing with age. It is divided into primary osteoporosis, related to menopause or aging, and secondary osteoporosis. The most common form is postmenopausal, which occurs in women during menopause and is linked to a decrease in estrogen. Over time, however, osteoporosis does not discriminate between genders and can affect both men and women. Secondary osteoporosis occurs either in patients with specific diseases (e.g. rheumatoid arthritis) or in patients who take medication that includes cortisone, antiepileptic pills, etc.
Osteoporosis is diagnosed by measuring bone density in the lumbar spine and the proximal end of the femur.
Risk factors for the development of osteoporosis are the patient’s family history, age over 50, female gender and therefore menopause, taking glucocorticoids, taking heparin, hyperparathyroidism, hyperthyroidism, smoking, alcohol, lack of physical exercise and a diet poor in calcium and vitamin D.
The peak bone mass is observed from 20 – 40 years of age, after 40 the gradual decrease in bone mass begins. Up to a point, osteopenia, i.e. low bone density, is a normal process, parallel to aging, as shown in the diagram below.
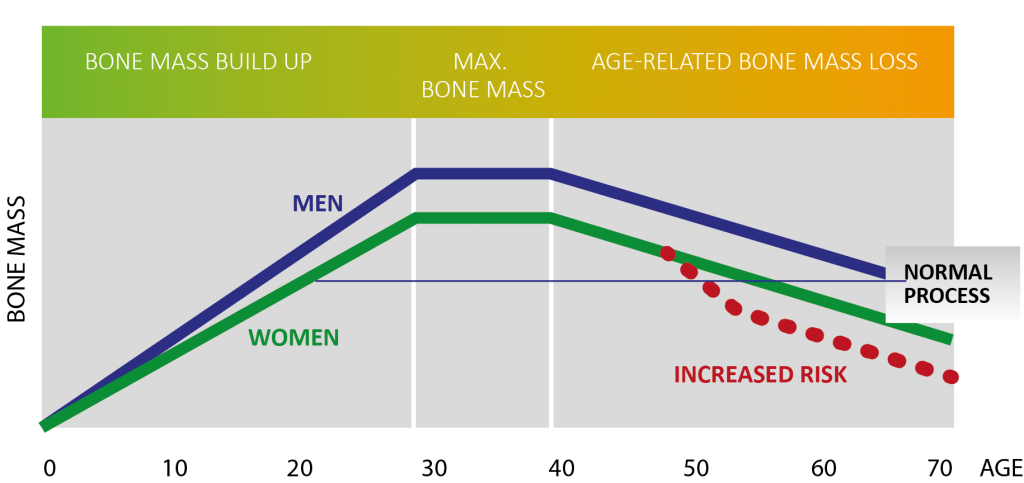
It is worth noting that the higher the maximum bone mass acquired during young adulthood, the slower its decrease and the likelihood of osteoporosis and fractures. Exercise in childhood and adolescence helps to increase peak bone density and consequently its slower decrease. However, this does not mean that we cannot inhibit its further decrease during osteoporosis or osteopenia through exercise. Exercise is a method that can have both preventive and therapeutic effects on osteoporosis. Bone is a living organism, which is in constant construction and reconstruction and to maintain skeletal health, a balance between bone resorption and bone formation is needed. Aerobic exercise during the week, exercise with progressive resistance increase 3-4 times a week and flexibility exercises have a beneficial effect on maintaining or even increasing bone density.
OSTEOPOROSIS AND NUTRITION
Considering that osteoporosis is a very common disease but one that we can prevent, it would be a good idea to include sufficient amounts of calcium and vitamin D in our daily diet.
Calcium deficiency is one of the most important causes of osteoporosis. Our body has 3 mechanisms to maintain stable calcium concentrations in the serum. When dietary calcium is reduced, we have a decrease in serum calcium and thus our body draws calcium from the bones. This gradually leads to a decrease in bone quality and density.
Vitamin D contributes to maximum calcium absorption. Therefore, its adequacy is very important in osteoporosis. People who are deficient do not absorb the calcium they take in through diet or calcium supplements. Vitamin D belongs to the fat-soluble vitamins, which means that the body does not eliminate it through urine, so attention needs to be paid to the amounts of intake. It is endogenously synthesized in the skin under the influence of the sun. Its dietary sources are fatty fish, eggs, liver, butter, and fortified milks.
Calcium requirements vary mainly depending on the age of the person.
The recommended amount of calcium intake is:

Calcium absorption from food
Calcium is not absorbed when we consume the entire recommended amount in a single meal, so it is recommended that it be proportionally distributed among daily meals.
Good sources of calcium include milk and its products, all cheeses, especially yellow cheeses, small fish that can be eaten with the bone, as well as salmon, nuts such as almonds and walnuts, dried beans, vegetables, especially broccoli and Chinese cabbage, as well as calcium-enriched foods such as breakfast cereals, plant-based milks, etc. Consuming dairy products 2 to 3 times a day covers the average daily calcium requirement.
Foods containing oxalates, such as spinach, green leafy vegetables, bulbs, chocolate, cocoa, prevent calcium absorption due to the oxalates they contain, so they should be consumed in moderate quantities and not at the same time as foods rich in calcium. In addition, increased alcohol and coffee consumption increases calcium excretion in the urine and prevents its deposition in the bones.
Patients taking thyroxine for hypothyroidism should take dairy products after 4 hours, due to poor absorption of thyroxine in combination with calcium.
Recent research also showed that low plasma vitamin C, compared to adequacy, was associated with lower peak hip bone mass, especially among postmenopausal women without estrogen therapy. It is also important to remember that vitamin C contributes to better absorption of calcium, as the presence of acidic substances (orange, lemon) changes the pH of the stomach.
As with most diseases, the best treatment for osteoporosis is prevention. Regular check-ups, exercise and a diet with adequate intake of calcium, vitamin D and vitamin C are the main factors that can enhance the development of bone mass and contribute to the management of osteoporosis.
SOURCES
Mangano KM, Noel SE, Dawson-Hughes B, Tucker KL., 2021. Sufficient Plasma Vitamin C Is Related to Greater Bone Mineral Density among Postmenopausal Women from the Boston Puerto Rican Health Study.
World Health Organization, Osteoporosis, 2011.
